
GOLDINCISION – A multifactor approach on cellulite treatment
Background: cellulite is characterized by changes in the surface of the skin with the presence of dimpling. The purpose of this study is to describe the technique called Goldncision, which combines local anesthesia, use of biostimulators, and detachment of fibrous septa with the goldenneedle and with the patient standing.
Methods: Observational multicenter study carried out in hundreds of patients with 10 years of follow-up with its own evaluation, treatment and follow-up protocol of the technique called Goldincision. Describe safety and effectiveness in addition to the satisfaction of medical staff and patients. This study was approved by the Research Ethics Committee of the Instituto de Cardiologia do Rio Grande do Sul / Fundação Universitária de Cardiologia/ IC/FUC under protocol number 30867114.3.0000.5333
Results: The level of satisfaction was considered excellent in patients treated with the technique to be described, as well as in the medical staff. Cases of seroma, hematoma and residual ecchymosis caused by hemosiderin were observed in some cases and absence of serious complications.
Conclusion: This study shows the effectiveness and safety of using the technique. Decompression of fat compartments and collagen biostimulation by particulate products seem to improve local circulation and, consequently, lymphedema, lipedema and venous edema, which, associated with septal detachment with the patient standing, allows immediate visualization of the result.
INTRODUCTION
Cellulite is a colloquial word used to denote the deposit of fat and fibrous tissue that cause dimples in the skin, but is misused, as it is not an inflammation or infection of the subcutaneous tissue1. The word originated in the French medical literature more than 150 years ago. The correct medical expression used for this condition is fibrosclerotic edematous panniculopathy or gynoid lipodystrophy. It is commonly known as a dermato-ogical change, however there are different theories to define the concept of cellulite. Cellulite is much more complex than a simple accumulation of fat2. The key factor is the presence of Estrogen so it occurs almost exclusively in post-pubertal women and is in fact present in 80-95% of women, in areas where fat is more predominantly under the presence of this hormone, such as buttocks, thighs and hips.
One of the theories for the appearance of cellulite refers to the occurrence of edema in the connective tissue that causes a large accumulation of water and generates cellulite. Another hypothesis is the compression of the venous and lymphatic systems that alters the microcirculation resulting in cellulite, mainly due to the obesity factor. A third possibility is that it may be associated with the difference of orientation on connective tissue fibers, which are perpendicular in female and oblique in men1,3, explaining the higher incidence of cellulite in women.
The appearance of cellulite can also be influenced by collagen reduction, stress, physical inactivity, obesity, heredity, hormonal contraceptives, age, gender, pregnancy, nutrition, among others factors 4.
Cellulite is characterized by dimpling overlying the Gluteal and Thigh regions, in addition to pain, especially in the more advanced stages. The formation of fat nodules, when increasing, result in the most advanced degrees. With this increase, its projection is opposed by the resistance strength of the trabeculae of conjunctive support. Treatments with topical and/or oral medications do not present very satisfactory results when used in advanced cellulite grades.
As not all the different treatments for cellulite have proven effectiveness, the Goldincision technique is performed being minimally invasive, done with an awake patient, with safety and effective results. The first step is the local anesthesia and bio stimulation with particulate products that helps to treat neocolagen and improvement of circulation, one of the causes of cellulite.
A standardized technique called “Goldincision” 5 with its own evaluation protocol, cellulite marking, local anesthesia, collagen biostimulation (before detachment), whose objective is to stimulate the general quality of the skin in the entire region and not punctual in cellulite, performed using a 10 cm x 18 G blunt microcannula distributed throughout the region, always with a moving cannula similar to liposuction, until this moment with the patient lying down.
The septum detachment must be performed with the patient standing up, allowing an accurate result, detaching just enough to level the irregularities, and only in the septa and not in all region.
In Goldincision is used a special needle called “Golden needle” for the section of these septa, releasing the traction they cause in the skin and stimulating the formation of collagen. During the procedure some blood vessels near septa can be sectioned, resulting in formation of transient ecchymosis with hematoma and seroma risk that are avoided with local compression during the first 24 hours. The patient should use a compressive shorts, suspend physical activities and do local massages for seven days.
PMMA (polymethylmetacrylate) is a polymer used as a filler presented in the form of synthetic microspheres with diameters between 40 and 60 micrometers mixed in a suspension vehicle that can be collagen, protic or crystalloid, used to perform the injection of the microspheres with microcannulas, without cuts or surgery.
(Figure 1)
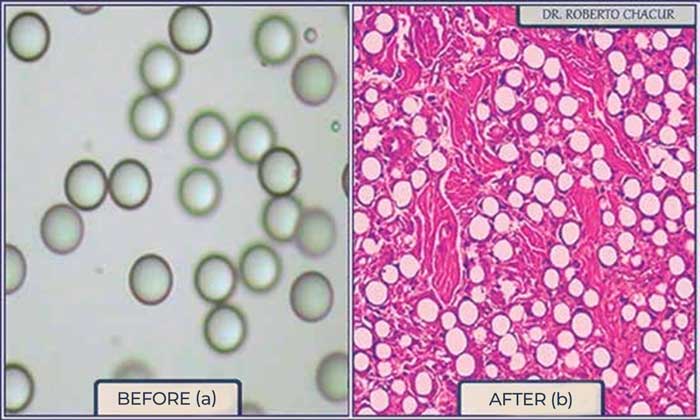
Commercial presentations can be 2%, 5%, 10%, 15% and 30%, depending on the concentration of PMMA. The product has permanent effect, with only vehicle absorption and tissue biostimulation around the particles such as in poly-L-lactic acid, calcium hydroxyapatite and polycaprolactone. PMMA can also be used as a biostimulator when applied in small quantities and spread evenly in the subdermal plane, due to its property of stimulating neocollagenesis through an controlled inflammatory response.
The microspheres are phagocytized and remain at the implant site, where there is a tissue reaction with giant cells around each microsphere, formation of collagen tissue and neovascularization, greatly improving the general aspect of the skin and even vascularization6.
Hundreds of patients underwent the technique, with satisfactory and proven safe results.
Cellulite affects almost all women, it is a very common complaint in our offices and its treatment is a real challenge, as it is due to the subcutaneous connective tissue involvement, with multifactorial causes that compromises the structure of adipose tissue. The technique called Goldincision has been established in Brazil due to its effectiveness and safety7.
As a multi-factor disease, involving circulation, lymphatic drainage deficient, localized fat, flaccidity and fibrous septa, cellulite treatment needs a broad approach aiming to combat each of these factors. Treatments with topical and / or oral medications do not present very satisfactory results when used in advanced degrees of cellulite, neither devices involving the most sophisticated technologies thus far, such as radio frequency, infrared, endermology and others7.
Described in the literature in 1977, Subcision consists of the fibrous septae detachment in select areas, but its technique, although achieves an apparent clinical improvement in some cases, leaves something to be desired. When performed there might be cases of new adherence of the same treated septum, non-efficacy, frequent complications such as seroma and bruising, in addition to limited results only in isolated areas without an improvement in flaccidity or relevant neocollagenesis.
Goldincision not only addresses fibrous septa, but also the general collagen bio-stimulation in the skin as a whole (and not in isolated points), improving sagging, circulation (telangiectasia induction) and lymphatic drainage. The way to perform the procedure from a holistic evaluation, in a static and dynamic way (with the patient in motion), including the definition of the ideal product and the treatment in an orthostatic position under local anesthesia, which is essential because in this position and only in this position we can assess the immediate result, as we need to take off as little as possible but enough to level out the irregularity. We cannot take off too much because we can cause a lump.
The post-procedure care that prevents adverse effects and is scarless, makes Goldincison a successful treatment with a great degree of satisfaction among patients.
Treatment starts after a complete analysis, informed consent and signed contract and a photographic record (in some cases video recording in motion). With the patient in an orthostatic position, first static and then in motion, all areas that will be addressed for detachment of the fibrous septa are marked in a detailed manner point-to-point. For greater comfort local anesthesia is injected with the patient in a decubitus position, with emphasis on these areas, using a solution with lidocaine at 2% dilution in a proportion of 1:1 respecting the maximum amount calculated by patient weight, usually 28 ml of solution in a 70 kg patient. This anesthetic is injected with a blunt tip microcannula for better comfort and safety, that prevents vascular trauma before the injection of the biostimulator product.
Local anesthesia is performed in the subcutaneous tissue of each fibrous septum, then the placement of a particulate filler is carried out. The product chosen must has a “firm” final result, such as calcium hydroxyapatite, polylactic acid, polycaprolactone or PMMA. Gel products like Hyaluronic Acid, Hydrogels like “Aqualift” and Biopolymers like “liquid silicone” are not used. Patients with those products in their body should also not be included when using this technique.
The chosen product must be homogeneously distributed in a three-dimensional form at different depths of the subcutaneous tissue, for bether neocolagen stimulation and no nodules, throughout the affected skin region and not only in fibrous depression, aiming for local collagen biostimulation with the objective of skin quality improvement, not volumization or cellulite filling. The product must be spread with a microcannula (10 cm and 18 G), always in motion, similar to liposuction, but in this case evenly distributed in the subdermis and different depths.
For better safety and distribution of the product, it must be placed before fibrous detachment, to avoid accumulation in the region below the cellulite that will be detached, and consequently nodular formation, and also to avoid possible embolism (common in liposculpture and much feared in fillings), because until then there will not be any vascular trauma.
After the anesthesia in the fibrous septum and biostimulation with particulate product in the region, the most artistic part depends on the doctor’s hand and must be performed with the patient in an orthostatic position with good lighting and using a Golden needle or a simple disposable needle. At the subcutaneous level a minimal detachment is carried out, enough to level the treated area point to point, always with the help of one or two assistants to maintain local compression. The irregularities are loosened in a deeper subcutaneous and sometimes with a “sandwich” technique at different depths to also avoid excessive detachment in a single plane, that can favor the formation of space for fluid accumulation (seroma) or even blood accumulation (hematoma).

- September 2021 published on PRS (Lauren A, Whipple): found in an ultrasound examination that in 97.6% of cases (169 of 173 irregularities) there was a fibrous septum, 84.4% with oblique or perpendicular orientation, 90% with superficial fascia origin, 11% related to vascular structure, more frequent in obese people or overweight.
This video demonstrates the identification of an oblique subcutaneous fascial band during the clinical evaluation of cellulite dimples.
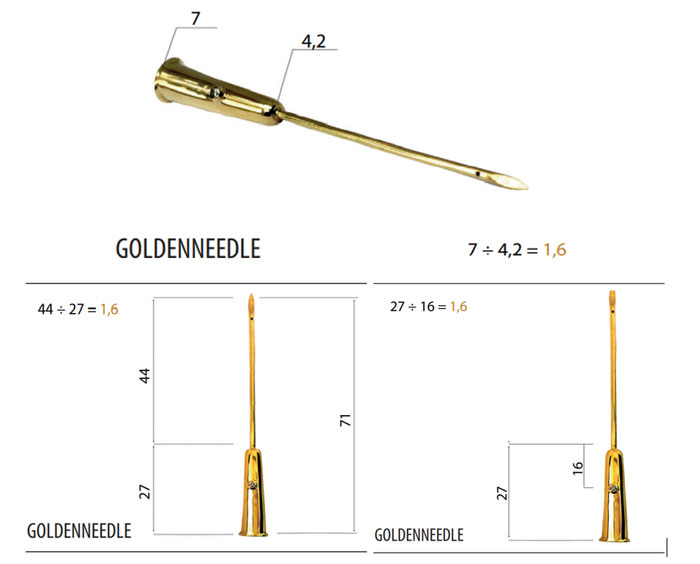
Developed following the golden ratio, the LeGolden needle is a prototype in gold with diamond, beveled for better bilateral cutting, with an orifice that allows the introduction of a local anesthetic to reduce even the slightest patient disconfort. The diamond helps to signal not only the hole but the cutting edges of the Golden needle.
(Figure 2)
(Figure 3)
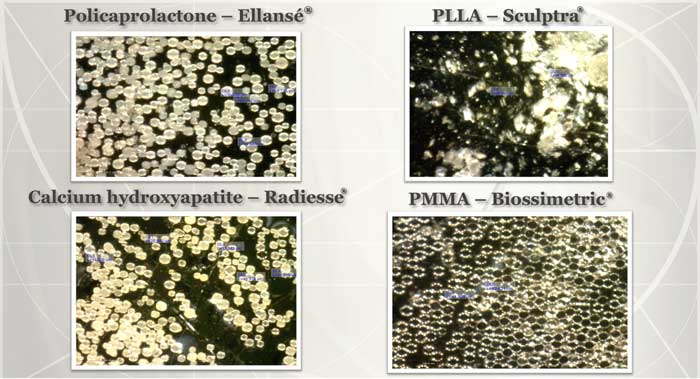
Microscopy of the main particulate products available on the market and used at Goldincision, such as polycaprolactone (Ellansé), calcium hydroxyapatite (Radiesse), polylactic Ac (Sculptra) and PMMA (Biossimetric and LinneaSafe).
(Figure 4)
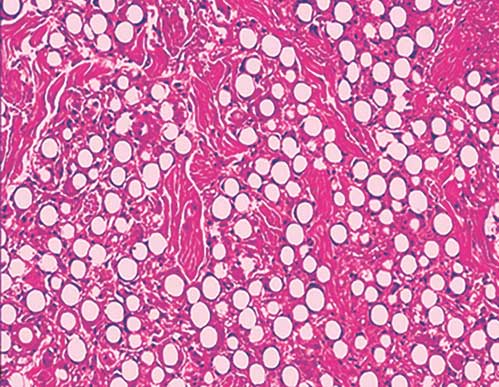
Tissue result of PMMA particles showing stability even after 10 years of application. Lemperle G, Sadick NS, Knapp TR, Lemperle SM. ArteFill permanent injectable for soft tissue augmentation: II. Indications and applications. Aesthetic Plast Surg. 2010;34(3):273-286. doi:10.1007/s00266-009-9414-0
(Figure 5)
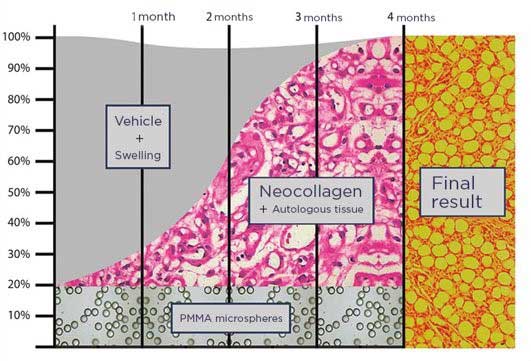
Illustrative design of the replacement of the vehicle such as the carboxymethylcellulose existing in particulate products such as polycaprolactone (Ellansé), calcium hydroxyapatite (Radiesse) and PMMA (Biossimetric or Linea Safe) by the patient’s own tissue. Something near 20-30% of the solution with particles of 40 microns in diameter work more as a substrate and tissue stimulator than properly fillers, maintaining a final volume very close to the infiltrate in the patient.
(Figure 6)
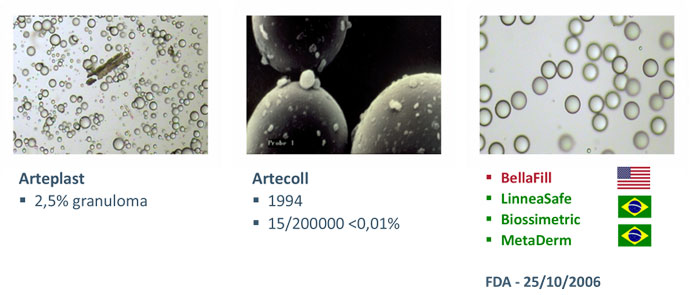
Evolution of PMMA in 30 years: first generation with particles of varying granulometry, second generation with good granulometry but an impure vehicle, third generation with good granulometry and without impurities.
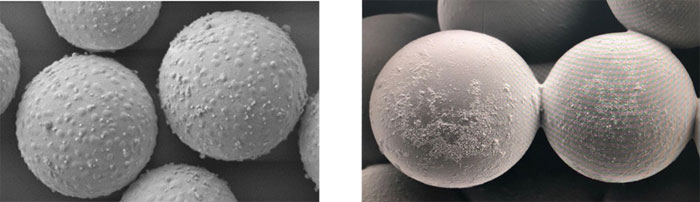
Today we see the development of a 4th generation of PMMA with perfect granulometry, without impurities and a textured surface instead of smooth, providing a larger area of contact with the tissue for faster tissue fixation and collagen biostimulation.
(Figure 7)

We have a post-treatment protocol to minimize the main adverse effects, such as hematoma and seroma, with local pressure being the most effective option for prevention. A compressive bandage is used for the first 24 hours in each of the areas where the fibrous detachment was performed. An elastic compression garment should readily available at the clinic for immediate use and used for a minimum of 7 days. When the bandage is removed at home, 24 hours after the procedure, an ointment should be used to treat ecchymosis and keep using the garment for a week.
TREATMENT
Initially, we fill an evaluation form taking the patient’s medical history, recording any previous treatment, we have the patient fill the informed consent and take photographs for documentation purposes. Both the filler and subcision procedures are performed in an outpatient environment, namely the doctor’s office, with local anesthesia. All the patients stayed awake and actively participated throughout the procedure, giving their opinion on the volume and location of the filler. Patients must stand up in front of a mirror to be marked, in decubitus, while local anesthesia is injected, with 2% lidocaine with a vasoconstrictor, diluted in saline 1:1. Next, we inject according to the patient’s wish around 3 to 10 ml of PMMA 10%, well spread in the regions to be treated, with a liposuction-like movement. It allows an even distribution of the product beneath the skin, in order to stimulate collagen production and improve the sagging look, ensuring a small local fill, to replenish the empty space created by the subcision.
LIPO-STIMULATION
In a liposuction procedure fat is removed symmetrically and in a well-distributed manner, to avoid the risk of subdermal irregularities where-as in lipo-stimulation we implant particulate products with a non-volumizing objective, as a neocollagenesis stimulator, as already discussed.
This technique can be performed with local anesthesia and using microcannulas, without cuts, stitches or scars. I usually use a 10 cm long microcannula, to minimize the need for more orifices, usually through a single orifice of 0.7 to 0.9 mm in the central gluteal region. This way, I manage to biostimulate the entire region; I first inject anesthesia and then inject the product; about 30 ml of particulate product (never gels like Aqualift or hyaluronic acid) on each buttock is adequate. We know that a product at 20%, whether polymethyl methacrylate or hydroxyapatite of calcium, or even polylactic acid (provided it is 40 microns in diameter) is enough to stimulate approximately 80% of the patient’s autologous tissue (4x more than its own volume)66,8, which is a collagen-rich connective tissue (a solid tissue) and for this reason we cannot let the product accumulate in the superficial plane, due to the risk of forming nodules, becoming palpable or even visible.
As with liposuction, the movement is the same; we can only inject the product with the cannula in motion; if we aspirate irregularly, the lipo will be irregular; if we lipo-stimulate irregularly, the product may be un-even. I carry out this procedure with PMMA at 30% because I can spread it thoroughly, as Ido it regularly, however I recommend that you start doing this procedure with PMMA 10%, minimizing the risk of nodules and/or irregularities in the injected area, whether in the face or body. I always advise augmentation and PMMA at 30% in deep planes, such as into the muscle or just above the bone. Injecting 45 ml intramuscularly will not have a pronounced neocollagen stimulation. For neocollagenesis and improvement in skin quality – not only due to a volume gain, which improves the skin through a lift effect, we need to inject some of the product, even if in small quantities, into the superficial subdermal plane, as I do in the face.
regularize the depression, and this can only be performed with the patient standing.This technique has proven to be very safe and effective.
DISCUSSION
Cellulitis, as this skin condition is commonly known, has the clinical appearance of an “orange peel” in its more advanced stages. In affected regions, the fat layer stiffens, affecting the adipose tissue. Cellulite has presence of fibrous band in 97.6%of cases9, associated with poor circulation and metabolic insufficiency10. In cellulite-free adipose tissues, there are spaces where fat moves freely beneath the skin. This clinical change in the skin and the risk of developing cellulite in the abdomen, buttocks and back of the thighs cannot be related only to obesity, as there are no limitations of regions for the development of cellulite in obese individuals.
New improved techniques are emerging in the field and they include multiple techniques to enhance the results. In 1997, the subcision technique was described for the treatment of cellulite grade 3 and 4 classificação de escala de Nürenberger e Müller
In “Goldincision” I use PMMA or other particulate filler for complementary purposes, aiming to achieve a synergic effect on collagen, volumization and neovascularization before subcison and at the same day, this makes this a safer procedure as the biostimulator product is infiltrated with atraumatic microcannula before any vascular injury, minimizing the risk of embolism and also reducing the risk of nodules, as the detachment prior to biostimulation can favor the accumulation of product in the “unglued space” previously providing the formation of nodules
. In this technique, after the photodocumentation, I mark and delineate areas with cellulite grades 3 and 4; then, with the patient in decubitus, I inject a local anesthesia with an atraumatic microcannula and then perform the lipo-stimulation with a particulate substance. The detachment of the fibrous septum must be performed with the patient standing to better identify the fibrous septa, always seeking to detach as deep as possible, and the minimum necessary to release the septum that pull the skin.
CONCLUSION
GOLDINCISION® is a registered name for a multifactorial treatment of cellulite, acting on several causes aiming at a more effective result and at all levels of cellulite, in addition to collagen remodeling, improving not only the irregular appearance but also acting on flaccidity, in addition to detachment of fibrous septa decompressing the fat compartments, relieving local pressure and improving microcirculation, water retention and lymphatic drainage, in other words, improving lipedema, lymphedema and venous edema. A technique created for the treatment of cellulite in all grades, involving an assessment, treatment, and monitoring protocol, in addition to the approval of products with proven quality with training of qualified professionals and frequent updating meetings between trained professionals.
It was possible to notice the significant improvement after the completion of “Goldincision” in the treatment of cellulite with a surprising degree of satisfaction of the patients and medical staff in addition to being safe with no significant adverse effects. “Goldincision” acts on several factors related to cellulite, such as fibrous septa detachment, subdermis structure and general improvement of skin appearance through collagen and improvement of local circulation induced by the presence of the biostimulator product. It was found that adiponectin (local vasodilator) is decreased in patients with cellulite11, strengthening the hypothesis that the improvement of this circulation improves the appearance, which is possible with the infiltration of biostimulators.
By detaching the “fibrosis” we are able to unzip the fat, reducing local pressure, improving blood flow, exchange of nutrients, tissue oxygenation and lymphatic drainage, in addition to neovascularization that the biostimulator is known to promote. All of these factors help us to have a successful result and an increasing demand for this treatment in our clinics.
REFERENCES
1. Nürnberger F, Müller G. So-called cellulite: an invented disease. J Dermatol Surg Oncol. 1978;4:221–229.
2. Emanuele E. Cellulite: Advances in treatment. Facts and controversies. Clin Dermatol. 2013;31:725–730.
3. Nurnberger, F. Practically important diseases of the subcutaneous fatty tissue (including so-called cellulite). Med. Welt. 1981, 32, 682–688.
4 De la Casa Almeida, M.; Suarez Serrano, C.; Rebollo Roldán, J.; Jiménez Rejano, J.J.; Cellulite’s aetiology: a review. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 273–278.
5. Subcision: a treatment for cellulite.Hexsel DM, Mazzuco R.Int J Dermatol. 2000 Jul;39(7):539-44. doi: 10.1046/j.1365-4362.2000.00020.x.PMID: 10940122.
6. Lemperle G, Morhenn V, Charrier U. Human histology and persistence of various injectable filler substances for soft tissue augmentation. Aesthetic Plast Surg. 2003;27:354–366; discussion 367.
7. 2. Rossi AB, Vergnanini AL. Cellulite: a review. J Eur Acad Dermatol Venereol. 2000;14:251–262.
8. Lemperle G, Sadick NS, Knapp TR, Lemperle SM. ArteFill permanent injectable for soft tissue augmentation: II. Indications and applications. Aesthetic Plast Surg. 2010 Jun;34(3):273-86. doi: 10.1007/s00266-009-9414-0. Epub 2009 Sep 29. PMID: 19787393; PMCID: PMC2872008.
9. Lauren A. Whipple, Craig T. Fournier, Adee J. Heiman, Amanda A. Awad, Malcolm Z. Roth, Sebastian Cotofana, Joseph A. Ricci. the Anatomical Basis of Cellulite Dimple Formation: An Ultrasound-Based Examination. Plastic and Reconstructive Surgery: September 2021 – Volume 148 – Issue 3 – p 375e-381e doi: 10.1097/PRS.0000000000008218.
10. Emanuele E, Minoretti P, Altabas K, Gaeta E, Altabas V. Adiponectin expression in subcutaneous adipose tissue is reduced in women with cellulite. Int J Dermatol. 2011;50:412–416.
11. Emanuele E, Minoretti P, Altabas K, Gaeta E, Altabas V. Adiponectin expression in subcutaneous adipose tissue is reduced in women with cellulite. Int J Dermatol. 2011;50:412–416.
FIGURE LEGENDS
Figure – 1. Comparison between PMMA microspheres before injection and in the muscular tissue surrounded by collagen fibers. Microscopic analysis, shown in the figure above, the PMMA particles without irregularities or impurities, while right side shows the stimulation of neocollagenesis by the presence of PMMA 10 years after implantation, as published by Lemperle.
Figure 2 – The golden ratio dimensions os the golden needle developed for Goldincinsion cellulite treatment.
Figure 3 – Microscopy of the main particulate products available on the market and used along with Goldincision, such as Polycaprolactone (Ellansé), Calcium hydroxyapatite (Radiesse), Polylactic Acid (Sculptra) and PMMA (Biossimetric and LinneaSafe).
Figure 4 – Illustrative design of the replacement of the injection vehicle such as the carboxymethylcellulose existing in particulate products. Near about 20-30% of the solution with particles of 40 microns in diameter such as Polycaprolactone (Ellansé), Calcium hydroxyapatite (Radiesse) and PMMA (Biossimetric or Linea Safe) stimulates 80% of the patient’s own tissue, working more as a substrate and tissue stimulator than proper fillers, maintaining a final volume very close to the amount injected in the patient.
Figure 5 – Evolution of PMMA in 30 years: first generation with particles of varying granulometry, second generation with good granulometry but an impure vehicle, third generation with good granulometry and without impurities.
Figure 6 – Nano textured particles of the PMMA 4th generation
Figure 7 – Case showing significant improvement in the skin quality due to the infiltration of particulate products. In the figure biostimulation with 20 ml of PMMA 30% on each side, always distributed with an atraumatic microcannula 10 cm x 18 g, moving in subcutaneous three-dimensionally (different depths) in a well distributed manner.
Figure 8 – The post-procedure care includes a compressive bandage in the first 24 hours and a compression garment for seven days.
Figure 9 – Improved skin quality by neocollagenesis resulting from a well-distributed and subcitaneos injection of polymethyl methacrylate (45 ml on each side) The volume injected improved not only the shape and firmness of the skin, but also the neocollagenesis (as already described). I also associated Goldincision subcutaneously. Photo taken after 30 days, still with some residual bruising. Exposure to sunlight needs to be avoided while there is ecchymosis.
Figure 10 – Goldincision (1 only session). additional sessions may be necessary.
Figure 11 – Before and after of the Goldincision treatment.
Figure 12 – Volumetry with PMMA, approximately 200 ml on each side in two steps. Not only it’s perceived a volumetric gain, but also a very significant skin enhancement in addition to Goldincision to release some fibrous septa.
Figure 13 – Before and after of the Goldincision treatment.
Figure 14 – Gluteal augmentation with subincision showing better body definition and skin quality.
Figure 15 – Before and after of the Goldincision treatment
Figure 16 – Before and after of the Goldincision treatment.
Figure 17 – General skin improvement by lipo-stimulation and a few Goldincision points.
Figure 18 – Gluteal definition by lipo-stimulation and fibrous detachment.
Figure 19 – Gluteal definition by lipo-stimulation and fibrous detachment.